Primary Leiomyoma of the Ureter: Report of a Case and Review of the Literature
Clinical History:
This 43 years old male was seen at the out patient clinic because of Rt. flank pain and gross hematuria. On an intravenous pyelograma, a smooth large filling defect was noted in the middle ureter accompanied by moderate hydroureter. The renal pelvis was unremarkable. A total nephroureterectomy was done.
Images:
-

Fig. 1
-

Fig. 2
-

Fig. 3
-
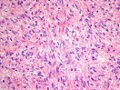
Fig. 4
-
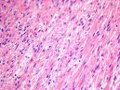
Fig. 5
-

Fig. 6
-
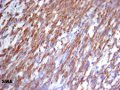
Fig. 7



Macro and Microscopic Description:
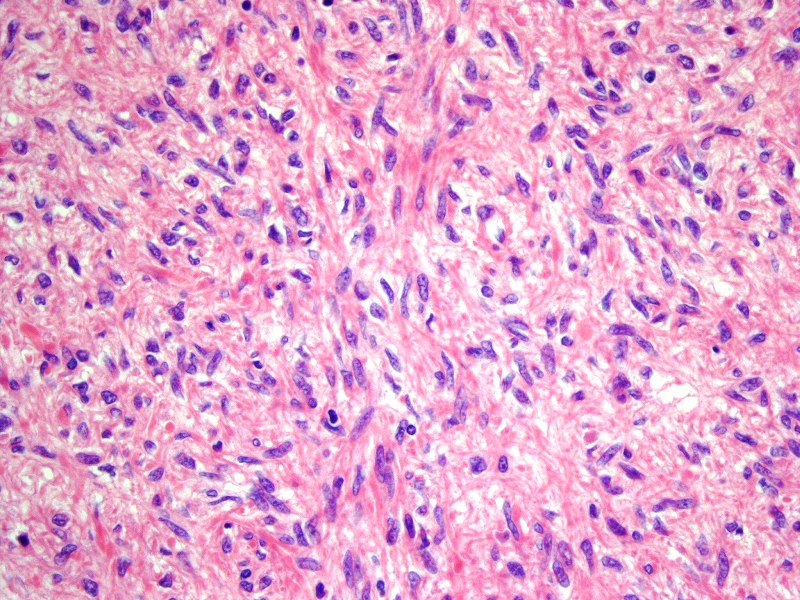
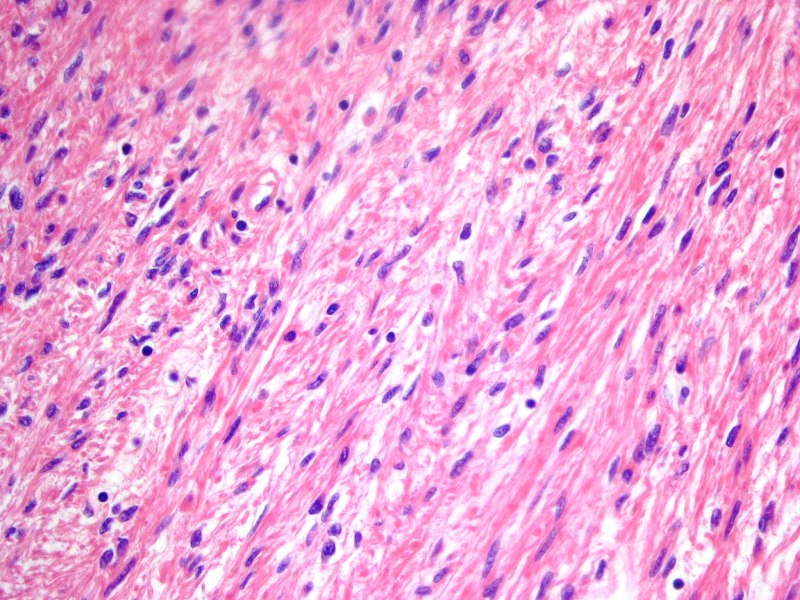
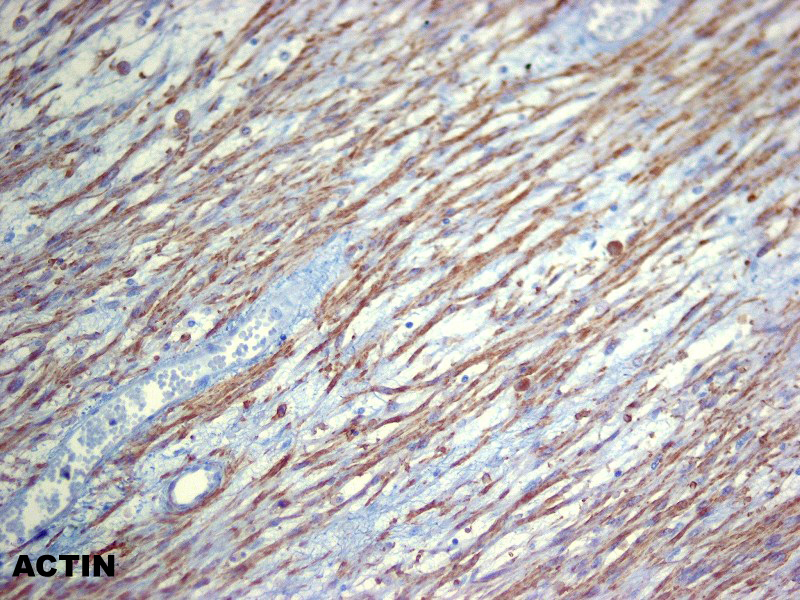
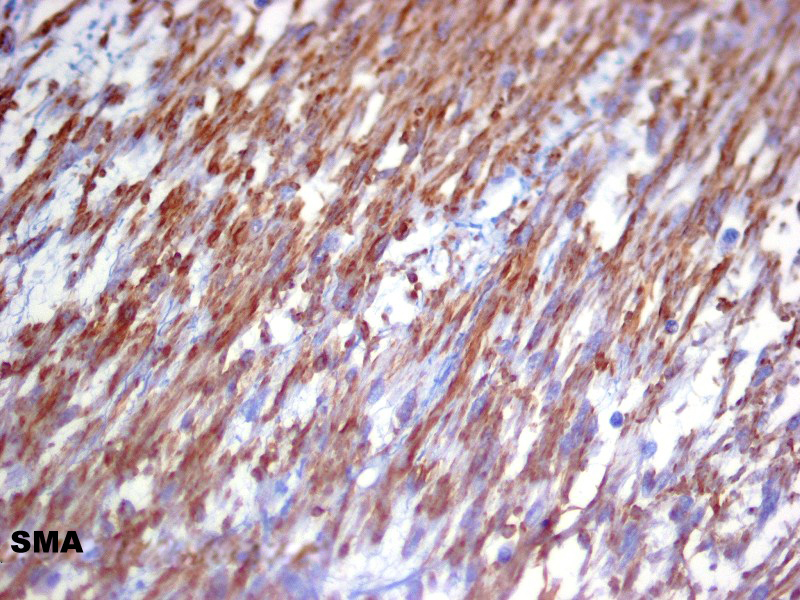
A large drum-stick shaped tumor is located in the ureter. On opening the ureter, a large, elongated, white, solid tumor fills the entire ureteral lumen and is attached to its wall (Figs. 1, 2, 3). Microscopic examination disclosed a spindle cell proliferation with cells of blunted, regular nuclei and an eosinophilic, fibrilar cytoplasm (Figs. 4, 5). No mitosis or necrotic foci were seen. There is a strong cytoplasmic immunoreactivity for actin (Fig. 6) and for specific smooth muscle actin (Fig. 7). S100 and CD34 are negative.
Diagnosis:
Primary Leiomyoma of the Ureter
Discussion:
Primary ureteral tumors are rare, and account for only 1% of all upper genitourinary tract neoplasms.
Benign ureteral lesions are even rarer representing approximately 20% of all ureteral tumors (1). Non epithelial benign mesodermal tumors are the rarest comprising less than 3% of all primary tumors of the ureter.
With the exception of the combined epithelial –fibrous tumors named fibroepithelial polyps that are frecuently found (2), only occasional examples of solitary neurofibroma (3) or in association with Von Recklinghausen neurofibromatosis are in the literature (4). Sporadic cases of primary hemangiomas are also recorded (5,6).
Primary leiomyomas of the ureter are uncommon and only 12 cases have been reported since the first case reported by Leighton in 1955 (7-18).
The age of the patients ranges from the 4th to the 5th decades of life. Only two cases are reported in children (9-16). The male gender is predominant 2:1. One case is associated with multiple endocrine neoplasia Type 1 (15).
Hydroureter, hydronephrosis, flank pain with hematuria, ureterocele and blood clot retention are the predominant symptomatology (10,14). Most tumors are located within the ureteral lumen in continuity with the muscle wall without extention to the renal pelvis.
References:
- Tanagho EA, McAninch JW. Tumors of the ureter,In Smith,s General Urology. Sixteen Edition,McGraw-Hill Companies,Inc,2004
- Turunc T, Kuzgunbay B, Canpolot T. Ureteral fibroepithelial polyps with calculi: a case series. Journal of Medical Case Reports 2008
- Blum MD, Babinson RR, Carter MF. Urologic manifestations of Von Recklinghausen neurofibromatosis Urology 1985; 26:209-217
- Varela-Duran J, Urdiales-Viedma M, Taboada-Blanco F, Cuevas C. Neurofibroma of the ureter. J Urol 1987; 138:1425-1426.
- Maestroni U, Dinale F, Fratteni A, Cortellini B. Ureteral hemangioma: a clinical case report. Acta Biomed 2005; 76:115-117
- Kim SJ,Jin cho H, Ha US,et al. Cavernous hemangioma of the ureter. Korean J Urol 2009; 50:192-194
- Leighton KM. Leiomyoma of the ureter. B J Urol 1955; 26:256-257
- Kao VC, Graff PW ,Rappaport H. Leiomyoma of the ureter. A histologically problematic rare tumor confirmed by immunohistochemical studies. Cancer 1969; 24:535-542
- Mondschein LJ, Sutton AP, Rothfeld SH. Leiomyoma of the ureter in a child the first reported case J Urol 1976;116: 516-518
- Sekar N, Nagrani B, Yadov RVS. Ureterocele with leiomyoma of the ureter. Br J Urol 1980; 52:400.
- Zaitoon MM. Leiomyoma of the ureter. Urology. 1986;28:50-51
- Cressenot O, Teillac P,et al . Leiomyoma of the urinary excretory tract. Ann Urol ( Paris) 1989; 23: 305-308
- Yashi M, Hashimoto S , Muraishi O, Tozuka K, Takere A . Leiomyoma of the ureter. Case report Urol Int 2000; 64:40-42
- Sha SA, Ranka P, Dodiya S, Jain R, Kadam G. Leiomyoma of ureter- a rare cause of intractable hematuria and clot retention. Indian J Urol 2004;20:181-182
- Ikota H, Tanimoto A, Komatsu H, Ozawa Y, Matsushita H. Ureteral leiomyoma Rausing hydronephrosis in Type 1 multiple endocrine neoplasia. Pathol Int 2004; 54:457-459
- Cobanoglu B, Ozucan IH , Yalcin O, Ergin E. Leiomyoma of the ureter in a child. Case report. Turk J Med Sci 2004; 34: 345-347
- Naruse K, Yamada Y, Aoki S, Taki T, Honda N, Iwafuchi H. A case of primary leiomyoma of the ureter. Int J Urol 2007; 14:248-250.
- Nouralizadeh A, Tabibi A, Mahmoudnejad N, Taheri M, Torbati PM. Partial uretectomy for a huge primary leiomyoma of the ureter. J Pak Med Assoc 2010;60:62-64
Author:
Dr. Juan José Segura Fonseca, Laboratorio de Patología y Citología Diagnóstica, S.A., San José, Costa Rica
